The Progesterone and GABA Link Explained
The week before your period, sounds feel louder. Conversations that normally wouldn’t bother you feel overwhelming. Your skin feels sensitive, tags on your clothes irritate you in ways they don’t the rest of the month. You’re on edge, snappy, reactive to everything. Your nervous system feels like it’s running at 150% capacity with no off switch.
You might describe it as feeling “wired,” anxious for no clear reason, or just unable to settle. Small stressors that you’d normally handle easily feel massive. You’re emotionally volatile, crying over things that wouldn’t make you tear up any other week. You feel overstimulated by normal levels of activity, noise, or social interaction.
This isn’t you being dramatic or overly sensitive. This is your brain losing its primary calming mechanism when progesterone drops.
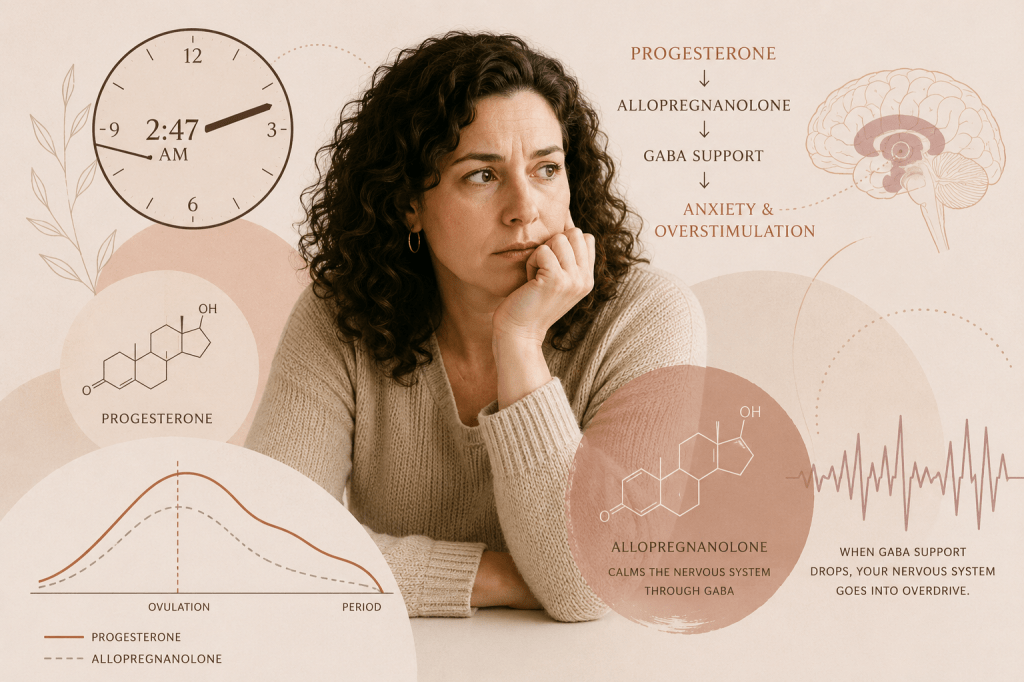
Here’s the specific neurochemistry: progesterone doesn’t just affect your reproductive system. It metabolizes into a compound called allopregnanolone, which is one of the most potent modulators of GABA-A receptors in your brain. GABA (gamma-aminobutyric acid) is your brain’s primary inhibitory neurotransmitter. It’s what keeps your nervous system calm, regulated, and able to filter out unnecessary stimulation (1).
During the luteal phase (the two weeks after ovulation), progesterone levels rise, which means allopregnanolone levels rise. Your brain is essentially bathed in this natural anxiolytic compound that’s keeping your nervous system smooth and regulated. You feel calm, stress doesn’t hit as hard, you can handle multiple demands without feeling overwhelmed.
Then progesterone drops rapidly right before your period. Within 24 to 48 hours, you lose most of that GABA support. Your brain goes from having an abundant, calming nervous system to having significantly less. This feels exactly like what you’re experiencing: anxiety, hypersensitivity, emotional reactivity, that wired feeling where you can’t settle.
I see this pattern in my practice constantly. Women describe it as feeling like their nervous system is “raw” or “exposed” the week before their period. They’re fine the rest of the month, but those few days before menstruation, they feel like a different person. Anxious, irritable, unable to regulate their emotions or handle normal stimulation.
This isn’t general PMS. This is a specific neurochemical response to progesterone withdrawal that can be understood, measured, and addressed.
The GABA Connection Nobody Explains
GABA is your brain’s brake pedal. It counterbalances glutamate, which is your brain’s gas pedal (the excitatory neurotransmitter). When GABA function is strong, you feel calm, you can handle stress, you sleep well, and your nervous system can downregulate when needed. When GABA function is impaired, you feel anxious, overstimulated, reactive, and unable to turn off your stress response.
Allopregnanolone (the progesterone metabolite) works by enhancing GABA-A receptor activity. It doesn’t just increase GABA levels; it makes your GABA receptors more sensitive and responsive to the GABA that’s present. This is actually more powerful than just having more GABA, because it amplifies the calming effect (2).
During the luteal phase, when progesterone and, therefore, allopregnanolone are elevated, your GABA system is functioning at maximum capacity. Your nervous system has significant calming support. This is why many women actually feel their best emotionally in the week or so after ovulation, before PMS symptoms set in. Their GABA system is optimized.
But when progesterone drops before menstruation, allopregnanolone levels plummet. This isn’t a gradual decline. It’s a rapid withdrawal that happens over one to two days. Your brain suddenly loses the compound that was amplifying its calming system.
The result is what researchers call “GABA withdrawal syndrome,” though it’s not typically named that in the context of the menstrual cycle. But the symptoms are identical to what happens when people withdraw from benzodiazepines (which also work on GABA-A receptors): anxiety, sensory hypersensitivity, emotional instability, insomnia, feeling wired and unable to relax (3).
Can’t figure out why you feel so anxious and overstimulated before your period?
Download The PMS Pattern Decoder to identify whether progesterone deficiency, GABA dysfunction, or another pattern is driving your symptoms.
Get your free assessment here.
Your brain is experiencing a neurochemical withdrawal from its primary calming compound. The anxiety isn’t in your head in the dismissive sense. It’s a predictable neurological response to losing GABA support.
Why Everything Feels Overwhelming and Too Loud
The sensory hypersensitivity that happens premenstrually for many women (sounds are too loud, lights are too bright, textures feel wrong, normal levels of activity feel overwhelming) is directly related to GABA’s role in sensory gating.
Sensory gating is your brain’s ability to filter out irrelevant stimuli and prioritize what’s important. Every second, your brain is receiving millions of sensory inputs. GABA is essential for deciding what to pay attention to and what to ignore. It dampens the “noise” so you can focus on the signal.
When GABA function is reduced because allopregnanolone has dropped, sensory gating is impaired. Your brain can’t filter as efficiently. Everything comes through at full volume. Sounds that would normally fade into background noise demand your attention. Visual stimuli feel more intense. Even physical sensations like clothing touching your skin or temperature changes feel more noticeable and irritating.
This isn’t you being oversensitive. This is your brain’s filtering system not working as well because it lost the neurochemical support it needs to function properly. Research on sensory processing and GABA consistently shows that GABA dysfunction impairs sensory gating and creates hypersensitivity to stimulation (4).
The practical impact: you feel overstimulated by normal life. A busy grocery store feels chaotic. Your kids playing at normal volume feels like too much noise. Social interactions that you’d normally enjoy feel draining. You need to retreat, be alone, reduce stimulation, because your nervous system can’t handle what it could handle easily two weeks ago.
The Emotional Volatility That Feels Out of Control
The emotional reactivity and mood swings that characterize this premenstrual pattern are also directly linked to GABA dysfunction.
GABA doesn’t just regulate anxiety and sensory processing. It’s also critical for emotional regulation. GABA activity in specific brain regions (particularly the amygdala and prefrontal cortex) determines how intensely you experience emotions and how well you can modulate your emotional responses.
When GABA function is strong, you can experience emotions without being overwhelmed by them. You feel sad or frustrated or irritated, but you can regulate those feelings, put them in perspective, and respond appropriately. When GABA function is impaired, emotions feel more intense and harder to control.
This is why women in this pattern describe crying over commercials, snapping at loved ones over minor things, feeling rage or despair that seems disproportionate to the trigger. The emotions themselves might be valid, but the intensity and the inability to regulate them is the GABA dysfunction.
Studies on emotional regulation and GABA show that reduced GABA function correlates with increased emotional reactivity, difficulty downregulating negative emotions, and heightened amygdala response to emotional stimuli (5). Your emotional responses aren’t exaggerated for no reason. Your brain’s emotional regulation system doesn’t have the neurochemical support it needs.
Why Some Women Experience This More Severely
Not every woman experiences severe premenstrual anxiety and nervous system dysregulation. Some women have minimal symptoms. Others are completely debilitated for several days every month. The difference comes down to several factors.
First, baseline progesterone levels matter. If progesterone isn’t rising adequately in the luteal phase (which can happen with anovulatory cycles, luteal phase defect, chronic stress, or declining ovarian function), you’re not getting as much allopregnanolone production. When progesterone drops, you’re dropping from a lower baseline, but the effect on your nervous system can be just as dramatic or even more so because you didn’t have robust GABA support to begin with.
Second, the rate of progesterone decline matters. Some women have a more gradual decline, which gives the brain time to adjust. Others have a very steep, rapid drop, which creates more severe withdrawal symptoms.
Third, baseline GABA function matters. If you already have compromised GABA function (from chronic stress, nutrient deficiencies, gut dysfunction affecting GABA production, genetic variations in GABA receptors or metabolism), you’re more vulnerable to the effects of losing allopregnanolone support. You’re starting from a deficit, so losing additional GABA support pushes you into symptomatic territory.
Fourth, the presence of other factors that affect nervous system regulation matters. If you’re dealing with blood sugar dysregulation (which affects neurotransmitter stability), inflammation (which impairs neurotransmitter production and receptor function), or thyroid dysfunction (which affects neurochemistry), the loss of progesterone’s GABA support is more impactful because your nervous system is already stressed.

Wondering why YOUR premenstrual anxiety is so severe when other women seem fine?
Download The PMS Pattern Decoder to identify which factors are making you more vulnerable. Get it here.
This is why telling women “PMS is normal, just deal with it” is so inadequate. The severity of symptoms reflects specific, measurable dysfunctions in hormone production, neurotransmitter metabolism, or nervous system resilience.
Why This Pattern Gets Worse with Stress and Age
Many women notice that premenstrual anxiety and nervous system dysregulation worsen during stressful periods of life or as they approach perimenopause. Both of these connections make perfect neurochemical sense.
Chronic stress depletes progesterone production. When you’re under sustained stress, your body prioritizes cortisol production over progesterone production because they share the same precursor (pregnenolone). This is called the “pregnenolone steal.” The more cortisol your body needs to produce to handle stress, the less pregnenolone is available to make progesterone.
Lower progesterone means lower allopregnanolone, which means less GABA support throughout the luteal phase. And when that already-reduced progesterone drops before menstruation, the effect is more severe because you’re dropping from a lower baseline.
Additionally, chronic stress directly impairs GABA receptor function and reduces GABA production. So you’re getting hit from both directions: less allopregnanolone from reduced progesterone, and impaired GABA function from the stress itself.
As women approach perimenopause, progesterone production becomes more erratic and generally declines before estrogen does. Cycles may become anovulatory (no ovulation, so no corpus luteum producing progesterone). Or the luteal phase shortens, so progesterone doesn’t rise as high or stay elevated as long.
The result: less GABA support from allopregnanolone, combined with greater nervous system vulnerability from age-related changes in neurotransmitter metabolism and receptor function. Premenstrual symptoms that were manageable in your 20s and 30s become severe in your 40s.
This isn’t you “getting worse at handling PMS.” This is progressive changes in hormone production and neurotransmitter function that require different support and intervention.
Why Magnesium and B6 Help (But Often Aren’t Enough)
If you’ve researched premenstrual anxiety, you’ve probably seen recommendations for magnesium and vitamin B6. These do help, and there’s good science behind why.
Magnesium is a cofactor for the enzyme that converts glutamate (excitatory) into GABA (calming). Without adequate magnesium, your brain can’t make enough GABA even if all the other raw materials are present. Magnesium also directly modulates GABA receptors, making them more responsive.
Vitamin B6 is required for the synthesis of multiple neurotransmitters, including GABA. B6 deficiency impairs GABA production, which makes you more vulnerable to the effects of progesterone withdrawal.
But here’s why supplementing these nutrients often helps but doesn’t completely resolve severe premenstrual anxiety: if the primary problem is loss of allopregnanolone’s amplification of GABA receptors, improving GABA production (with magnesium and B6) only addresses part of the issue. You might have adequate GABA, but without allopregnanolone, your GABA receptors aren’t as responsive to it.
This is why women often say, “I take magnesium and B6, and it helps a little, but I still feel terrible before my period.” The nutrients are supporting baseline GABA function, which is helpful. But they’re not replacing the allopregnanolone that your brain is missing.
To fully address this pattern, we need to either support progesterone production so there’s more allopregnanolone, provide direct GABA support during the vulnerable window, or use compounds that can substitute for allopregnanolone’s GABA-enhancing effects.
Want to know exactly what YOUR body needs to stabilize mood and nervous system function throughout your cycle? Download The PMS Pattern Decoder for the complete breakdown.
What Actually Needs to Be Assessed
When someone comes to me with premenstrual anxiety, hypersensitivity, and that wired feeling, I need to understand their progesterone production, GABA function, and what other factors might be compromising nervous system resilience.
That means looking at:
- DUTCH test (Dried Urine Test for Comprehensive Hormones) to see progesterone levels throughout the cycle and progesterone metabolites. This shows me if progesterone is rising adequately in the luteal phase and whether it’s being metabolized properly. If progesterone is low or the metabolites are off, that explains inadequate allopregnanolone production.
- Neurotransmitter testing (urine or serum) to assess GABA levels and the glutamate-to-GABA ratio. If GABA is low or glutamate is high relative to GABA, the nervous system is already in an excitatory state, making progesterone withdrawal more impactful.
- Nutrient testing for magnesium, B6, zinc, and other cofactors required for neurotransmitter synthesis and metabolism. Deficiencies in any of these impair GABA production and receptor function.
- Cortisol rhythm via DUTCH or salivary testing to assess if chronic stress is depleting progesterone production through the pregnenolone steal. If cortisol is chronically elevated or the rhythm is dysregulated, that’s affecting progesterone availability.
- Thyroid function including free T3 and reverse T3, because thyroid hormone affects both progesterone production and neurotransmitter metabolism. Hypothyroidism or poor T4-to-T3 conversion often contributes to both hormonal and neurochemical dysfunction.
- Organic acids testing to look at neurotransmitter metabolites and assess whether breakdown pathways are functioning properly. Sometimes GABA production is adequate, but it’s being metabolized too quickly, which creates functional deficiency.
But beyond labs, I’m listening carefully to the symptom pattern. When in your cycle do symptoms appear? Is it exactly when progesterone should be dropping, or earlier? How severe are the symptoms? Do you have other signs of low progesterone (short luteal phase, spotting before period, difficulty conceiving)? Do you have signs of high stress or HPA axis dysfunction? The pattern tells me which interventions will be most effective.
How We Actually Restore Nervous System Stability
Once I understand what’s driving the progesterone-GABA dysfunction, the intervention is targeted to address the specific mechanism.
If progesterone production is inadequate, we’re supporting the body’s ability to make progesterone. This might include addressing chronic stress to reduce the pregnenolone steal, ensuring adequate cholesterol intake (progesterone is made from cholesterol), supporting ovulation if cycles are anovulatory, and sometimes using bioidentical progesterone supplementation in the luteal phase if production is insufficient.
If GABA production or function is impaired, we’re providing the nutrients required for GABA synthesis (magnesium, B6, taurine, theanine), supporting gut health (the gut produces GABA and provides precursors for brain GABA synthesis), and sometimes using GABA-supporting compounds like passionflower, valerian, or theanine during the luteal phase.
If the HPA axis is dysregulated and depleting progesterone, we’re addressing the stress response with adaptogenic herbs, nervous system regulation practices, and ensuring adequate recovery and sleep. We might use phosphatidylserine to lower evening cortisol if it’s elevated, or support cortisol production if it’s depleted.
If nutrient deficiencies are impairing neurotransmitter function, we’re repleting those nutrients with therapeutic doses, not just dietary amounts. Magnesium glycinate (for GABA support and nervous system calming), methylated B6, zinc, and ensuring adequate protein intake for amino acid availability.
We’re also often using strategic timing of interventions. Some nutrients and compounds are most effective when started several days before symptoms typically appear, so we’re preventing the GABA withdrawal rather than trying to treat it once it’s already happening.
The common thread: we’re giving the body what it needs to either maintain adequate progesterone production (and therefore allopregnanolone), support GABA function independently of allopregnanolone, or both.
What Happens When GABA Support Is Restored
When we successfully support progesterone production and GABA function, the premenstrual anxiety and nervous system dysregulation improve dramatically.
The wired, overstimulated feeling disappears. You can handle normal levels of stimulation throughout your cycle. Grocery stores, social events, and family activities don’t feel overwhelming anymore.
Sensory sensitivity normalizes. Sounds, lights, textures, and other sensory inputs don’t feel amplified or irritating before your period.
Emotional regulation returns. You feel emotions proportionately and can modulate your responses. You’re not crying over small things or snapping at people you love. Your mood stays stable through your entire cycle.
Anxiety decreases significantly or resolves. The baseline anxiety that showed up every month before your period just stops appearing. You feel calm and capable of handling stress throughout your cycle.
Sleep improves because the anxious, wired feeling that made it hard to fall asleep or caused nighttime waking resolves. Your nervous system can downregulate properly at night.
Most women describe feeling like they “got themselves back” or say they didn’t realize how much the premenstrual anxiety was affecting their quality of life until it was gone.
Let’s Decode Your Premenstrual Pattern
If you’re recognizing yourself in this description (premenstrual anxiety, feeling wired and overstimulated, sensory hypersensitivity, emotional volatility that appears like clockwork before your period), you need to understand your specific progesterone production and GABA function, not just accept that this is normal PMS.
On a Connection Call, here’s what we do: I walk through your complete symptom pattern with specific attention to timing, severity, and what helps or worsens symptoms. When do they appear relative to your cycle? How long do they last? What have you tried?
We review any testing you’ve already had done. Most women have had basic hormone testing that showed “normal” results, but that testing doesn’t capture progesterone metabolites, GABA function, or the nutrients required for nervous system stability.
I explain which specific tests would reveal your particular pattern of progesterone-GABA dysfunction and what’s driving it.
And we map out what a protocol would look like to restore stable nervous system function throughout your entire cycle, not just manage symptoms when they appear.
These calls are comprehensive, usually 30 minutes long, because hormone-neurotransmitter connections are nuanced and require an understanding of multiple systems. The cost of the call is applied to any of my offerings after the call.
If you’re ready to stop accepting severe premenstrual anxiety as normal and start understanding the specific neurochemistry creating your symptoms, you can schedule a Connection Call. We’ll identify your pattern and what it takes to stabilize it.
You’re not being oversensitive. You’re not failing at stress management. Your brain is experiencing a predictable neurochemical withdrawal from losing progesterone’s GABA support. Let’s give your nervous system what it needs to stay stable all month long.
References
- Schiller CE, Meltzer-Brody S, Rubinow DR. The role of reproductive hormones in postpartum depression. CNS Spectr. 2015;20(1):48-59. doi:10.1017/S1092852914000480
- Backstrom T, Bixo M, Johansson M, et al. Allopregnanolone and mood disorders. Prog Neurobiol. 2014;113:88-94. doi:10.1016/j.pneurobio.2013.07.005
- Sundstrom Poromaa I, Gingnell M. Menstrual cycle influence on cognitive function and emotion processing-from a reproductive perspective. Front Neurosci. 2014;8:380. doi:10.3389/fnins.2014.00380
- Epperson CN, Steiner M, Hartlage SA, et al. Premenstrual dysphoric disorder: evidence for a new category for DSM-5. Am J Psychiatry. 2012;169(5):465-475. doi:10.1176/appi.ajp.2012.11081302
- Terner JM, de Wit H. Menstrual cycle phase and responses to drugs of abuse in humans. Drug Alcohol Depend. 2006;84(1):1-13. doi:10.1016/j.drugalcdep.2005.12.007

Leave a comment